Risk Paradigm Refined
Risk Paradigm Refined
MONICA Monograph and Multimedia Sourcebook
The sourcebook of the World Health Organization-supported Multinational Monitoring of Trends and Determinants in Cardiovascular Disease (MONICA), is an archive of the seminal study papers, a summary of the data, and documentation of the major study events and all its [click for more]Acceptance, extension, and applications of the CVD risk factor paradigm characterized the Modern Era. The risk factor concept, formulated from solid epidemiological work of the Early Era, stimulated much academic and professional activity in CVD prevention.
Researchers sought new CVD risk factors and elaborated on the traditional ones by ethnicity, age, and gender. Policymakers developed national and international policy to support prevention research and training. This resulted in medical and public health programs to reduce CVD risk. First, however, the clinical medical establishment required experimental “proof” by explanatory preventive trials prior to its endosement of epidemiologists’ recommendations for preventive action. Major new prevention trials of single and multiple risk factors got underway. Simultaneously, CVD mortality rates fell dramatically and steadily across much of industrial society, documented by the WHO MONICA project.
Next Slide Next GalleryRisk Factor Paradigm Extended
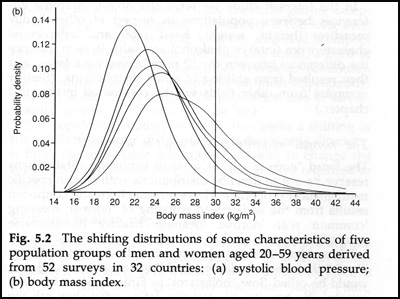
Prevalence of overweight based on variable distributions of body mass index (BMI) in 5 populations of men and women ages 20-59
A classic graphic by Geoffrey Rose illustrating the relation between the distribution of BMI and the prevalence of “overweight.” The small separation among population distributions of BMI results in large differences in the prevalence of this criterion of overweight (BMI=/>30). [click for more]Researchers extended the risk factor paradigm beyond cholesterol, blood pressure, diet and smoking. Estimates of individual risk, both relative and absolute, were further refined and the proportion of population CVD events attributable to the traditional risk factors estimated. Most CVD cases in a population were found to derive not from the extreme risk categories but from the center of the distribution of risk levels generally called “normal.” The range of risk factor values of a population determines the proportion found at any arbitrary clinical “diagnosis” of high risk. (see graphic)
Thus, a more efficient approach to universal CVD prevention was suggested: a relatively small shift in the entire population distribution of risk factors downward by public health promotion.
Next Slide Next GalleryGender
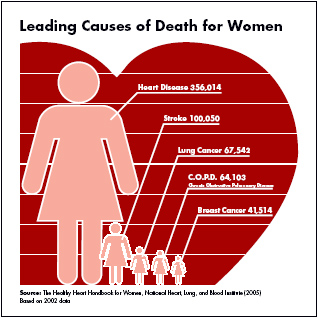
Leading Causes of Death for Women
Epidemiological CVD studies on women, mostly introduced in the Modern Era, revealed that women and men differ in CVD risk, manifestations, diagnosis, treatment, and prognosis. [click for more]The broad public health orientation of the original USPHS designers of the Framingham Study led to their inclusion of women in the Framingham cohort. Women were not studied in a number of the new epidemiological undertakings, including the Seven Countries Study among cohorts of rural men. In 1950, CVD events were 4 to 5 times rarer in women at comparable ages, therefore much larger samples were required. Biases in some cultures about physical examinations, disrobing, exercising, and blood letting in women were strong and negative. In the modern era, studies revealed that women are different: different in risk, manifestations, diagnosis, treatment, and survival of vascular events.
Next Slide Next GalleryNew Preventive Trials
New generations of preventive trials in the Modern Era looked to “prove” experimentally that the risk factors were indeed “causal” or at least in the chain of causation. Researchers measured the effect of reducing particular risk factors on the rates of disease. Cholesterol lowering by drugs, particularly the Lipid Research Centers Primary Prevention Trial of the 1980s and later Statin trials, finally and sufficiently “proved” the causal role in atherosclerosis of certain blood lipoproteins and brought wide acceptance of lipid modification as a medical and public health prevention strategy.
Similarly, the reduction in heart attack and stroke rates in trials of anti-hypertensive drugs adequately “proved” the causal role of blood pressure and confirmed the combined medical-population strategy of hypertension control. Paradoxically, vigorous public health measures against cigarette smoking were advanced by the medical and the public health community without requiring experimental “proof” from controlled trials.
Next Slide Next Gallery