“It Isn’t Always Fun.” – Elegance in Medicine
Lecture
Presented in the Rutherford Aris Lecture Series, University of Minnesota, October 9, 1999, and revised for
The Alexander Langmuir Lecture, American Epidemiological Society, Tampa, March 16, 2000
I invite you to muse with me about Elegance in Medicine. Please be forewarned that my musings will avoid the excitement and elegance to be found these days in molecular biology and in high-tech modern medical care, mainly because they are beyond my ken.
You may ask at the outset, why search at all for Elegance in Medicine? We cannot force together science and the humanities. But surely we can try to conduct science within artful lives. Doing science and making art not only complement each other, they intertwine, as I hope to show.
But relating Medicine and Elegance is not well-worn intellectual ground as is, for example, elegance in language or in physics, or in architecture or cosmology. Indeed, one wonders whether we in medicine are condemned obligatorily to inelegance because of our rude origins in animism, shamanism, voodooism, missionary evangelism, and social Darwinism. It must be admitted that physicians come in a direct line from herbalists and from sorcerer-poisoners, from tattooers, trephiners, circumcisers, embalmers, bone-setters, bleeders, and purgers, and from barbers who also cut for stone.
Moreover, one cannot deny, traditional medicine has been characterized over the centuries by pedantic detail, petrified formalism, arcane spiritualism, and an unholy reverence for authority.
How can we possibly rise — elegant — above such origins?
I propose that we must simply try.
Facing this challenge in a new millennium, I turned naturally to the Worldwide Web to search on “elegance + medicine,” where I was provided a mere 1.5 million hits! At the top of the list was “Bare Elegance,” which I opened enthusiastically to find an advertisement for a so-called upscale gentlemen’s club. The next association of elegance and medicine was an ad for “elegant natural hairpieces.” The web search deteriorated thereafter.
Elsewhere, I learned early that Elegance, above all, is Excellence and that things elegant are also:
concise and precise;
non-trivial, uncomplicated, unexpected, and illuminating.
Things elegant are:
creative, balanced, round, and graceful.
They are also:
logical, strong, dexterous, and eloquent.
They may be:
serendipitous, revolutionary, witty, and wise.
And they can be:
durable, charitable, and even loving.
Then, I solicited ideas from friends, including Garrison Keillor, Minnesota’s national sage of Lake Wobegon fame, who responded as follows:
“When one uses the word elegance, Midwesterners misinterpret it as involving candlelight and expensive sauce-laden dinners, while the essence of the term — effective simplicity — gets lost.” I found his “effective simplicity” concise, complete, and useful.
Spencer-Brown, the mathematician, is more elaborate: “. . .
elegance is achieved by condensing as much as is needed into as little as is needed, and so making that little as free from irrelevance (or from elaboration) as is allowed by the necessity of writing it out and reading it with ease and without error.” Which seems elegant indeed except for the length of that sentence.
Ockham’s Razor is widely held as an elegant principle in science. William of Ockham, 13th century Franciscan logician [known as doctor invincibilis] said that: “entia non sunt multiplicanda praeter nesessitate,” or “entities should not be multiplied unnecessarily.” His principle holds that the simplest, most parsimonious explanation for a phenomenon is likely to be the correct one (and, one might add, the more elegant one).
A colleague, Jeff Sullivan, suggested that elegant contributions to knowledge are the ones that force us to abandon a prior body of knowledge (Einstein), or are concepts that fundamentally alter the world (Newton’s calculus).
Whatever the definition, it seems that Elegance is in the eye of the beholder. Moreover, Elegance is not to be sought after, like Truth, but rather is recognized — or bestowed — honorifically.
Finally, it seems that Elegance is only approached — rarely realized.
Perhaps then it would be more appropriate for us to consider these proposals as candidates for Elegance.
Candidates for Elegance in Medicine, including
people, sayings, concepts, and events
Louis Pasteur: “There are not two sciences; there is only science and the application of science. And these two activities are linked as the fruit is to the tree.”
Clinicians and epidemiologists accept Pasteur’s elegant idea easily. Bench scientists seem to have great trouble with it.
Rudolf Virchow: The scholarly 19th century experimental physiologist-pathologist, gave us elegant insights into the origins of epidemics, saying: “Mass diseases are always due to profound disturbances of human culture.”
Think of poverty, rats, fleas, and the medieval plague; or think of crowding, cheap gin, social depravity, and tuberculosis in early industrial London. Nowadays, think of the explosive spread of AIDS worldwide. These disturbances of culture are reflected by changes in mass behavior resulting in distortions of lifestyle and, eventually, in mass diseases.
Lewis Thomas: This most eloquent cell-watcher and Mahler-listener in American medicine today said: “Biological science, with medicine bobbing somewhere in its wake, is under way, but only just under way. At the moment we are an ignorant species, flummoxed by the puzzles of who we are, where we came from, and what we are for. It is a gamble to bet on science for moving ahead, but it is, in my view, the only game in town.”
Lewis Thomas’s elegant advocacy of science suffices not for me to forgive his once sardonic definition of epidemiology as merely “leafing through death certificates!”
Serendipity
Serendipity might be a hallmark of elegance: the transformation of a fleeting or recurrent observation, an accident, into a new concept or discovery:
• Percival Pott encountered an unheard-of cancer, cancer of the scrotum, in 18th century London chimney sweeps and made the serendipitous leap of logic to “soot cancer,” the first example of carcinogenesis due to products of carbon combustion.
• John Hunter, also in 18th century London, recognized the relation between emotions and the crushing chest pain and sudden death of angina pectoris. He even predicted his own downfall after he developed angina, saying: “My life is in the hands of any rascal who chooses to annoy or tease me.” Soon after, when contradicted one day in a public meeting, he had to be led from the chamber with angina, only to die a few minutes later.
• Alexander Fleming, after a time, no longer ignored the clear circles in his bacterial cultures surrounding growths of mold contaminants. The mold, of course, was Penicillium.
• Kaposi’s Tumor, the first serendipitous association by dermatologists of these unsightly dusky tumors of the skin with sexually promiscuous young men, led rapidly to the identification of AIDS and its causal agent, the HIV.
• Other examples of serendipity in medicine are legion: connecting cow pox to small pox, fermentation to Pasteurization, olive oil to longevity, marathon running to levels of HDL (or “good cholesterol,”) and Tampons to toxic shock, not to mention the dramatic events, some serendipitous, of the race to discover the double helix.
But surely I push too far. Serendipity, like genius, may be 97 percent perspiration, 3 percent inspiration.
William Harvey, for example, in the 17th century, estimated from many simple and tedious measurements of cardiac input and output in animals he bled experimentally, that perpetual return of blood to the heart was required. He elegantly proposed that the heart had to be an automatic pump to raise fluid above its original level — thus, modern hydraulics — and that filling of the heart and arteries was by impetus, rather than Galen’s centuries-old view that it was by cardiac dilatation and suction. Furthermore, Harvey, knowing nothing about capillaries, and observing arteries to enter tissues filled with bright red blood and leave with dark, elegantly assumed that capillaries existed — because they had to.
I read Rabelais’s Gargantua and Pantagruel as a senior in medical school and wondered about his profound knowledge of medicine. His life is an elegant testament to a fruitful union of medicine and the humanities. In the Renaissance world of three professions, theology, law, and medicine, Rabelais trained in and practiced all three. In theology he challenged the orthodoxy of the Theological Faculty of Paris (the Sorbonne). He displaced the Old Testament idea of illness as divine punishment with a new evangelical hope; and he considered some forms of illness the sign of a troubled spirit. He replaced the Arabic medicine of his day with the humanism of Hippocrates and Galen, translating and teaching from their original writings in Greek. Medicine became the medium for his reflections on the human condition in which he promulgated the hygiene of the ancient Greeks, a newer strategy of prevention, and a quite modern policy of public health.
Rabelais is best known today, of course, as the powerful author whose allegory, satire, and polemic allowed him to attack medical frauds of his day while at the same time battling social illnesses. Charmingly, Rabelais restored the ancient linkage of medicine with comedy, seeking what he termed, “the joy that is the proper occupation of man.”
Epidemiology
Epidemiology adds systematic observation to serendipity, making precise counts of defined cases, then demonstrating relationships among characteristics of the cases versus characteristics of the population in which they occur.
John Snow, a legendary physician-surgeon-anesthetist, painstakingly collected facts about cholera deaths in relation to sources of drinking water during the epidemics in London’s Soho from 1849 to 1854, some 30 years before the vibrio organism of cholera was identified. The legendary part of his work was the experiment of removing the pump handle, which he persuaded the St. James parish Board of Guardians to do. The deaths, already falling, then plummeted. His theory was confirmed, though he was never sure that removing the pump handle was responsible.
The elegance of Snow’s work lay in the clarity of his questions, the simplicity of his investigative methods, and the seamless character of his approach: first seeking mortality data from the General Register, then interviewing families of the deceased, then postulating the water-borne mechanism, taking action by petitioning the Board about the pump; prompt publication of a report and then carrying out follow-up studies in a London population of 300,000, which he divided into those supplied with water containing London sewage and those having water “quite free from such impurity.” This was followed by elaboration of procedures to take during an epidemic and those that should be taken beforehand. Finally, came his on-going, hands-on, confident activism for public health program and policy based on sound epidemiology.
Milton Terris has wondered why we in this country eulogize John Snow as the “nearly perfect model” of the epidemiologist when we have our own Joseph Goldberger; the model being, of course: the patient data collector, accurate observer, logical analyst, and courageous worker who forwards conclusions against the authoritative opinions of the day. The effective simplicity of such an approach is demonstrated elegantly in Goldberger’s classic studies of pellagra.
To return to the times of John Snow, William Farr was, for more than 40 years in the mid-1800s, Director of Statistics in the General Registrar’s Office in London. He determined the nature and quality of all data collected on births, deaths, and marriages, and controlled their analysis. With an equal avidity for denominators, Farr directed the census for many years. The elegance of his contributions came from exploiting all these data with skill and imagination, making regular and special reports giving objective analyses, then adding his forceful opinions and arguments for recommended action. If a part of elegance is durability, Farr developed the methods for calculating excess respiratory and total deaths in influenza epidemics, methods still widely used to quantify the impact of epidemics on mortality.
C.E.A. Winslow links neatly into a chain from Farr and Snow to Langmuir and D.A. Henderson. The elegance of Winslow’s career and character is reflected in his 1944 editorial: “Who Killed Cock Robin?” in which he demonstrated that the amazing achievement of a 40 percent reduction in U.S. mortality rates since 1900 was due almost entirely to public health efforts, sanitation and the economy rather than to medical care and practice. We now can give somewhat more credit to medical practice for the gains in mortality of the last half of the 20th century, but, of course, nowhere near the lion’s share medicine likes to claim.
Alex Langmuir, whose philosophy and methods were in a direct line from Farr, called Farr “the greatest of statistical epidemiologists.” They shared a faith “that natural laws govern the occurrence of diseases, that these laws are discoverable by orderly epidemiologic inquiry, and that, when discovered, the causes of epidemics admit to a great extent to remedy.” Langmuir’s methods and strategies were direct forerunners of the surveillance and control programs of D.A. Henderson and William Foege — the millennial elegance (my term, my italics) of the Smallpox Eradication Program.
Burkitt’s Lymphoma
The story of Burkitt’s Lymphoma (BL) included Denis Burkitt’s laborious survey by Land Rover across central Africa to describe the distribution of this variable disease among youth. He established the equatorial high-risk area for BL, having particular temperature and rainfall characteristics and bounded both by latitude and altitude. The territory mapped closely with the known range of the anopheles mosquito, which raised the initial query whether the mosquito was a vector for the spread of the Epstein-Barr virus (already shown to be incorporated in BL cell genomes and suspected as a causal agent).
Anopheles turned out not to be a carrier. Rather, malaria in young children itself proved to be the strong predictor of development of BL. According to John Potter, this led to the hypothesis that the antigenic stimulus of the malarial parasite, which keeps changing its expressed surface antigens and thus evades immune elimination, in fact, stresses the immune system continuously. In the face of hyperproliferation, sooner or later a malignant clone grows out. “The EBV,” says Potter, “has a nasty habit of incorporating and immortalizing the relevant cells.” This hypothesis turned out to be pretty much how it, Burkitt’s Lymphoma, works.
The story of Burkitt’s Lymphoma involves, again according to Potter, “lovely interactions among descriptive and ecologic epidemiology, parasite biology, immune system biology, molecular biology and analytic epidemiology. The elegance emerges from one man, Guy de The, being able to contribute to and integrate these phenomena as the pieces emerged.”
Risk Factors
The modern concept of risk factors is a viable candidate, a concept elegant both for its simplicity and for its wide impact and utility. [“risk factor” is here defined as a measurable element in the chain of disease causation and a strong, significant, and independent predictor of future risk]. The concept developed from tedious observations in long-term systematic cohort and cross-cultural studies, especially the Framingham Study and the Seven Countries Study. The major risk factors for heart, vascular, and lung diseases and for many cancers are now well established in practice and in public health.
* * *
Before I propose other candidates for elegance in medicine and epidemiology let me set the frame and attempt a metaphor of the three major research disciplines in medicine: laboratory-experimental, clinical-pathological, and population-epidemiological, which I label here:
The Three Beauties
Consider the Three Beauties of Medical Science:
The Baroque Beauty of Biology;
The Modern Beauty of the Clinic;
The Classic Beauty of Epidemiology.
Ponder their separate missions:
The search for universal truths and specific mechanisms in the laboratory; for uniquely individual phenomena and their causes and cures in the clinic; and for mass phenomena, their causes and prevention in the population at large.
Each muse is distinctive and each complements the others. None is inherently superior to the others. Broadest understanding derives from all three taken together. The greatest strength comes from the ability to employ each according to the stage of knowledge and the question asked.
Finally, each beauty must be fostered for all to flourish!
Simple Distribution Curves
Let us look then at more candidates for elegance coming from the discipline of “classic beauty,” that is, epidemiology and population studies.
The first is from a study of heart attacks in 16 areas of seven countries among men of the same age engaged in traditional rural lifestyles and having large contrasts in diet [The Seven Countries Study, initiated in 1957, by Ancel Keys from Minnesota ].
I find elegant the distribution curves to follow, for their simplicity and effectiveness and for how much they tell us:
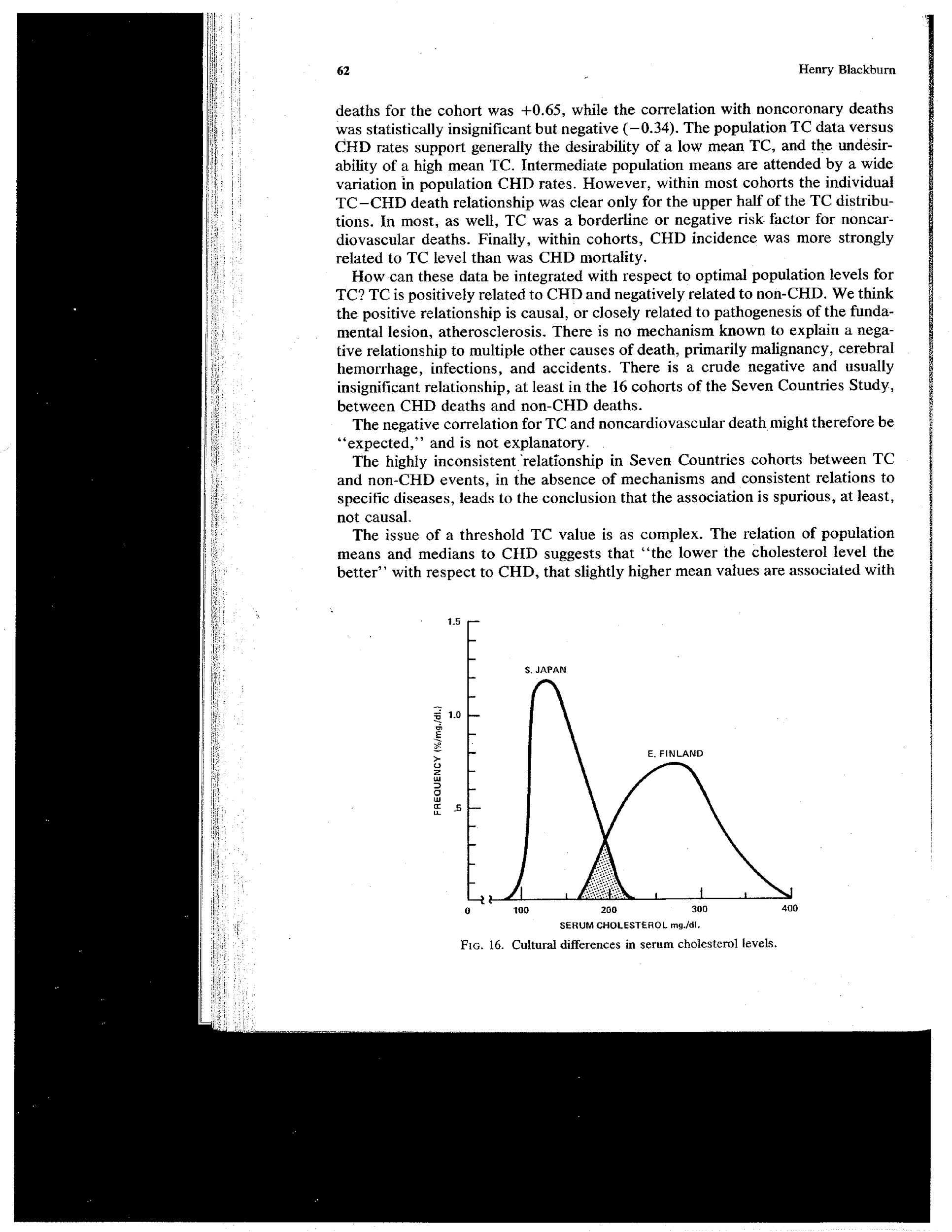
Serum Cholesterol Distributions in Rural Japanese and Finnish Men in the Seven Countries Study
The blood cholesterol levels of these population samples in Japan and Finland are almost wholly disparate. Their elegant curves call into question what is a normal cholesterol level. They indicate that the lower the average value the greater the central tendency, the higher the mean, the wider the spread and greater the skewness toward high values. They imply that nature or genes relate to the position of an individual in the population distribution, but that nurture determines the spatial configuration of the population data. The latter is confirmed by rapid time trends in risk and disease levels in these same populations as well as by migrant studies and by experimental shifts in risk factor distributions upon dietary manipulations among the same individuals.
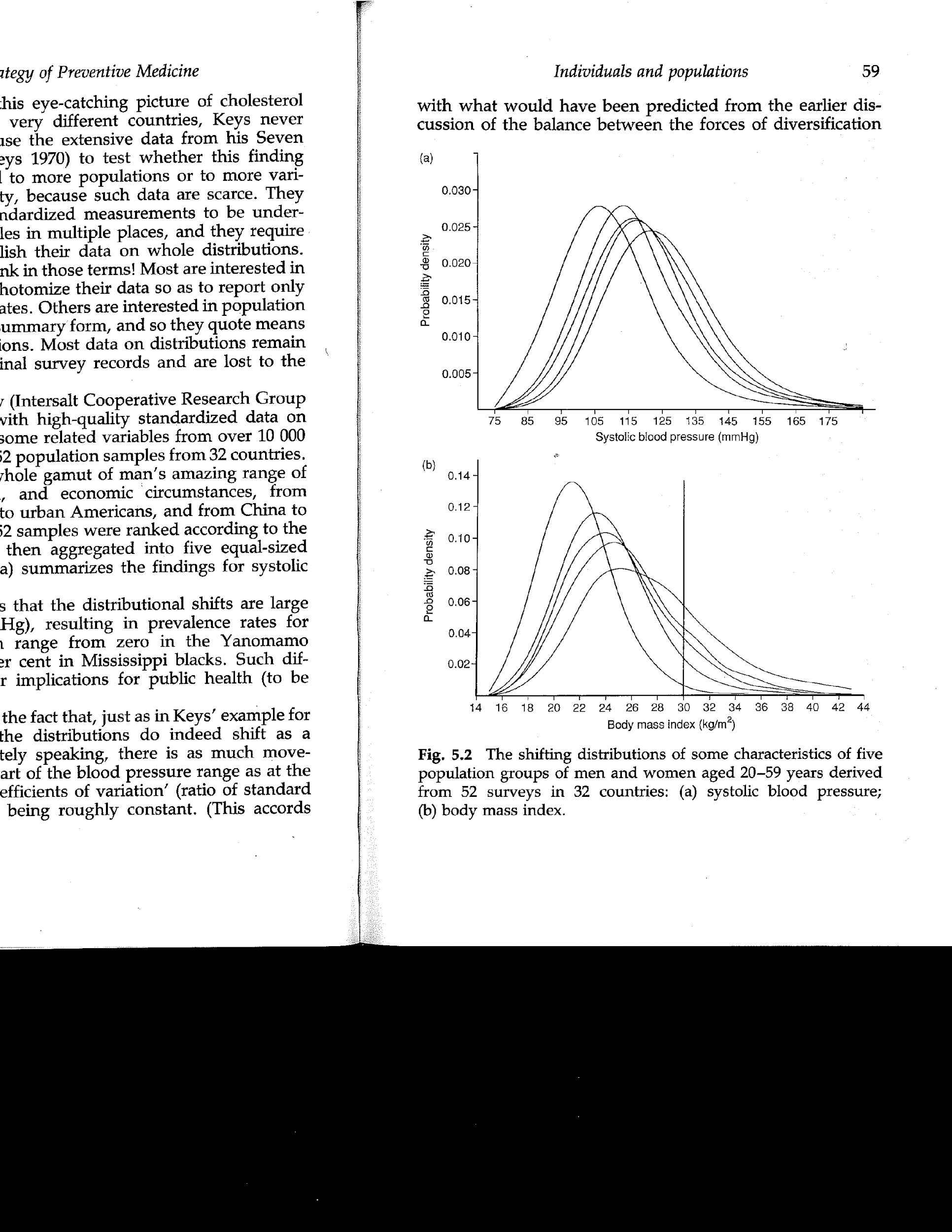
Distribution of Body Mass Index in Five Different Populations. From G. Rose’s 1990 Keys Lecture
Above is a family of simple distribution curves of body mass index values among five populations arrayed in order of their average value and where we see the phenomenon of skewness. When we do the “medical thing” that we seem to have to do, that is, pigeonhole people as overweight or not (as sick or well, as high or low risk, as normal or abnormal) by some arbitrary breakpoint (in this case a body mass index of 30), the proportion of people labeled high risk in the population varies from about 2 percent to as much as 30 percent. These curves illustrates the obvious: that the most effective way to reduce high risk would be to shift the whole distribution leftward using population-wide strategies, presumably dealing simultaneously with the variously defined high risk segment by using medical strategies.
These simple distributions contribute to a major and, I find, elegant public health concept about the common diseases of industrial societies. We are dealing, as Geoff Rose has called them, with “sick and well populations” in addition to sick and well individuals.
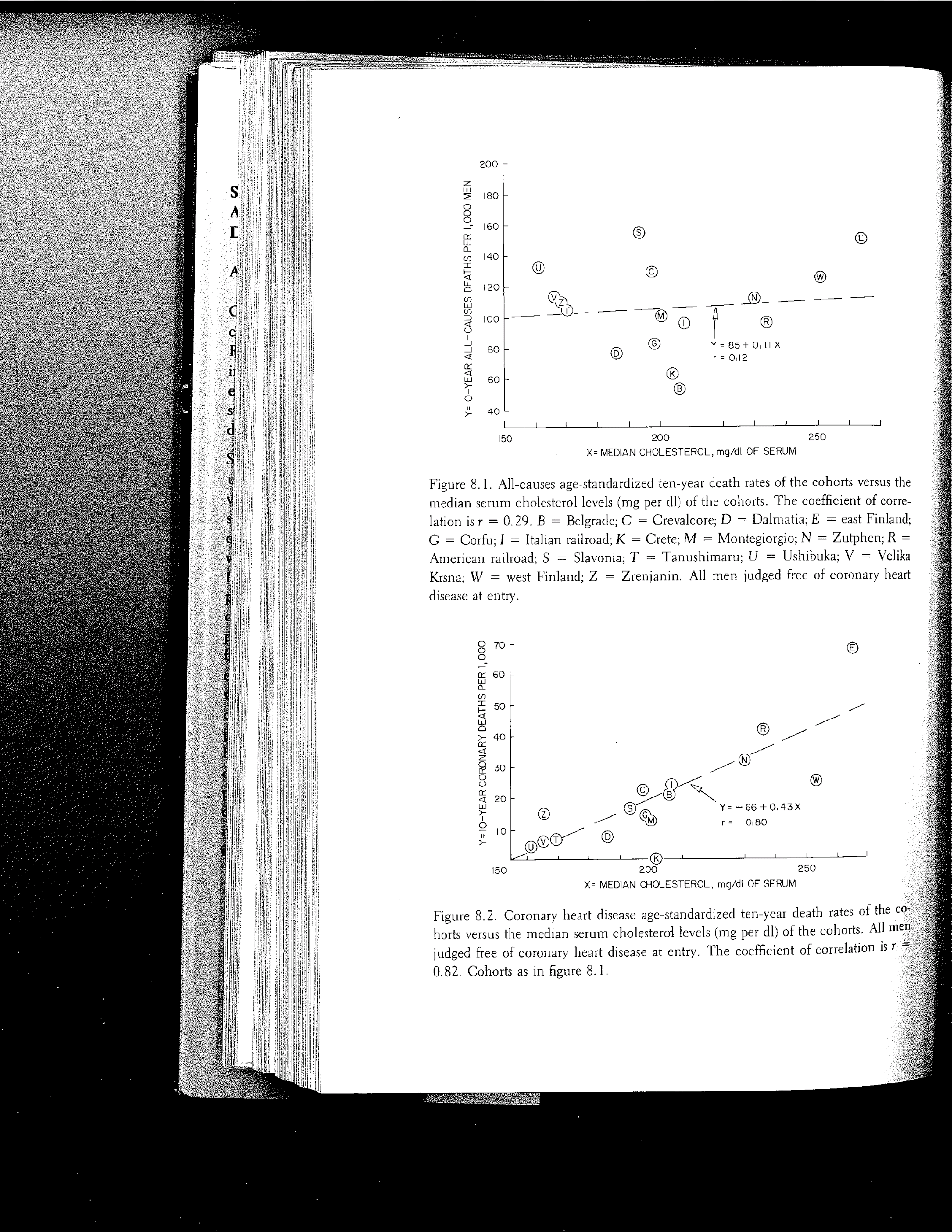
Mean Serum Cholesterol Level in 14 Populations of the Seven
Countries Study, versus 10-year CHD Incidence, from Keys, 1980
Regression equations
Some think that an ultimate goal of science is to construct regressions. Here we examine simple linear correlations of the more dangerous ecologic kind, on the grand but simple scale of whole populations differing widely in diet, between mean cholesterol level, and 10-year coronary death rate. Of course, we accept or reject this general relation as causal depending on other and congruent evidence from the clinic and the laboratory. And fully as exciting as the clear relationship shown here are instances of departure from the prediction, or the exception that tests the rule. This can lead, in turn, to new ideas and questions. (Examples here are: extra-high-and low-risk Finns at points E and W; extra-low-risk Cretans at point K.)
Attributable Risk (AR)
AR is an elegant concept. A geometrically expanding region of high relative risk affects only a small fraction of a generally high-risk population; most of the excess cases come from the center not the extremes of the risk distribution.
Criteria for Causal Inference
The following familiar criteria for causal inference from statistical associations, developed by Sir Bradford Hill and elaborated by others, are a candidate for Elegance because of their clarity, cogency, and great utility:
Strength,
Gradation,
Temporality,
Prediction,
Independence,
Consistency,
Plausibility or congruence.
These criteria applied to epidemiological associations make the lie of know-it-all claims such as, “statistics don’t count;” “statistics can prove nothing,” or, “statistics lie.” To the extent the above criteria are met, inference of causality increases.
Multivariate equations
Multivariate equations are elegant when we think of the cumbersome cross-tabulations they replace. They allow looks at relationships between outcomes and a risk factor after adjustment for the effects of other risk factors with which they may be correlated.
Meta-analysis
Pooled analysis and meta-analyses are also candidates for elegance. One of the first such in medicine was this 1960s equation based on pooling of data from some 60-odd metabolic ward experiments varying dietary fat and cholesterol content, with calorie intake held constant. This equation, called the “Keys” (or Minnesota) Equation, is a candidate for elegance for its simplicity and utility and durability. For 35 years it has provided our best estimate of the effects of a known dietary change on blood cholesterol level.
∆Chol. = 1.35(2∆S – ∆P) + 1.5∆Z
Where:
∆Chol. = Change in Serum Cholesterol level in mg. percent
∆S = Change in Saturated Fatty Acids in percent of calories
∆P = Change in Polyunsaturated Fatty Acids in percent
∆Z = Square root of change in Dietary Chol. mg./1000 Kcal.
The Keys Equation says in essence that saturated fatty acids raise blood cholesterol level twice the degree that polyunsaturates lower it, and that blood cholesterol is additionally moved,
but in a curvilinear fashion, according to the square root of change in dietary cholesterol intake.
I found it serendipitously elegant when art imitated science in this cartoon from the mid-1970s. Subsequently I corresponded with the cartoonist, who, of course, had no inkling of the Keys Equation or of the square root relationship between blood cholesterol level and dietary cholesterol intake, for which egg yolks are, of course, the major source!
Experiments
Much of modern medicine has grown out of the experimental tradition formalized and diffused by Claude Bernard. The following elegant curves from the dietary experiments of Marc Hegsted, for example, show the contrasting distributions of blood cholesterol values, but this time instead of between populations they are in the same individuals under separate experimental conditions: diets of different fatty acid composition. To me, these curves are meaningful, simple, and elegant:
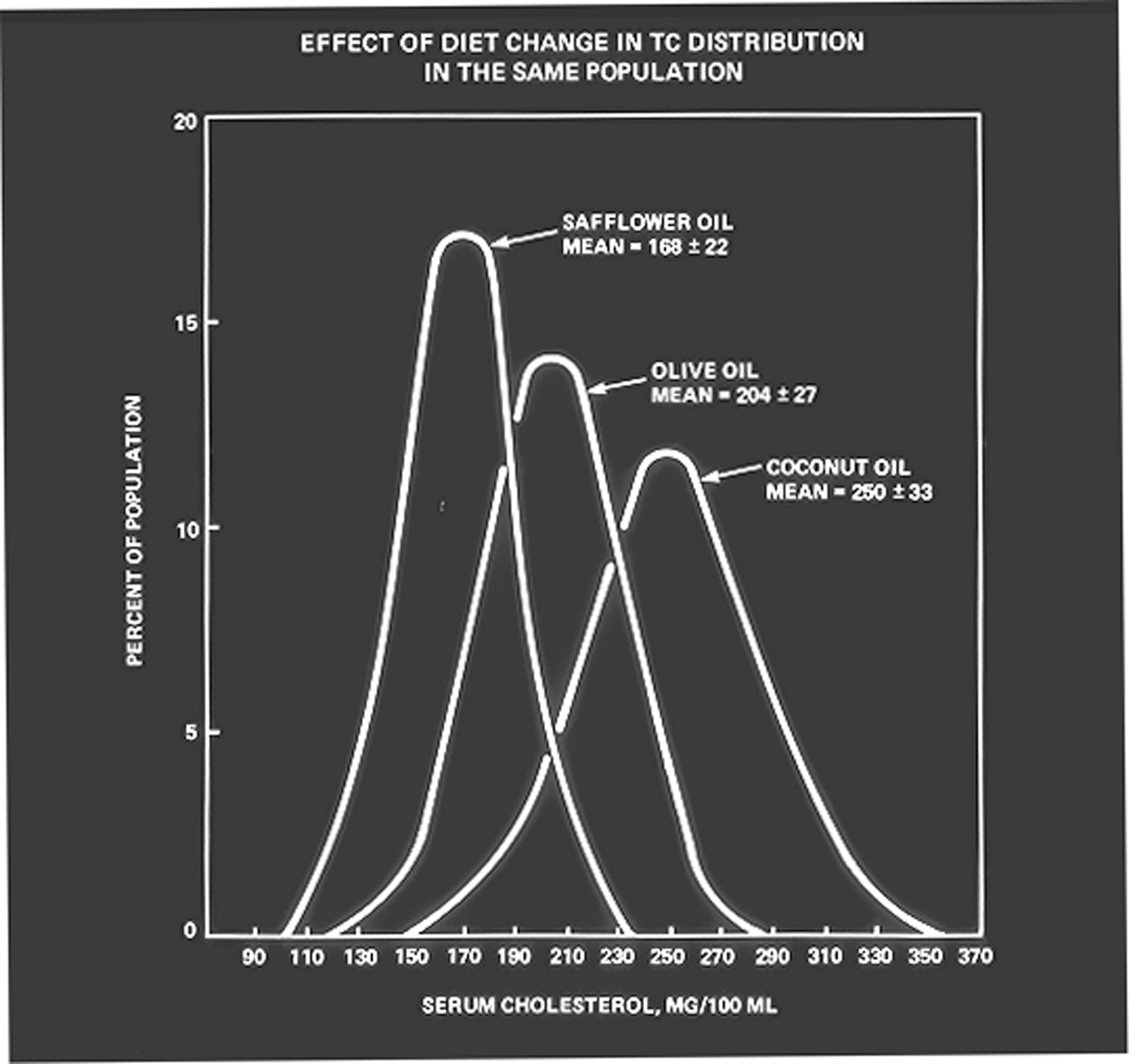
Total Serum Cholesterol Distribution of the Same Individuals on Experimental Diets of Different Fatty Acid Configuration. From Hegsted.
Randomized Clinical Trials (RCT)
The RCT is one of the more elegant things in all of modern medicine, providing, if imperfectly, the best way we have of testing causal influences, other factors held constant.
In sum, all of these simple distribution curves and associations have led to a whole new and, I suggest, elegant view and strategy of disease prevention, the population view. They have clearly changed our view of who needs prevention and when.
Specific Epidemiological Studies
Listing specific elegant epidemiologic investigations and investigators surely would create errors of omission and commission. With several collaborators, I am preparing a comprehensive history of the pioneering studies in CVD epidemiology and prevention in which we hope to do justice to the more seminal and elegant studies. Whenever I ask people their choice of elegant studies at the close of this lecture, the responses are broad and varied.
Modern diagnosis and therapy in the clinic and the beauty and elegance of molecular biology are areas I deliberately shortchanged here, only because of my unfamiliarity with them.