Epidemiology as a Bridge
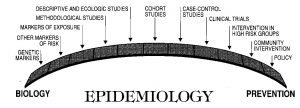
Graphic courtesy of John Potter, 1986, Fred Hutchinson Research Center, Seattle.
The figure above portrays a broad idea about the function of epidemiology: a discipline serving as a bridge between biology and the public health. It recognizes all medical disciplines and investigative strategies, while it provides a population (species-wide) view of causality and prevention. It seeks out the appropriate research discipline according to the stage of knowledge and acknowledges the research method appropriate to the scientific question. It is pointed toward health applications and not exclusively academic, theory-gelled, method-focused, or otherwise narrow in its view of what is real (“Big-E”) epidemiology.(1)
It recognizes epidemiology as the basic science of prevention and as a sound and often elegant means of translating scientific evidence into the fruits of personal and public health. It is entrepreneurial and catholic in its approaches to questions deemed important to the public health; it is neither elitist nor cloistered nor preoccupied with itself.
Epidemiology can be the stronger bridge to support and join biology and preventive action, from genes and their markers, through risk factors and exposures, to methods for descriptive and analytical studies in populations (including ecologic studies among populations), to long-term prospective studies of individual risk among cohorts, to case-control comparisons, to randomized clinical trials and preventive trials among the high risk, to community interventions, and eventually to public health outcomes, surveillance, health policy and prevention programs.
Epidemiologists are the specialists more frequently called upon to evaluate evidence for real effects at the population level, to quantify the actual risk attributable to an exposure, and to synthesize the evidence systematically – most needed when the evidence is incomplete – to formulate sound, evidence-based recommendations to the public.
Such is the understanding, philosophy, and approach of a multi-disciplinary program of “Little-e” epidemiology, based in sound biology and social science, nurtured in the field, joined with statistics, ecology, social medicine, and cultural anthropology, strengthened by group theory and advanced methods and computation, and tested in far-flung researches among contrasting cultures. It is in no ivory tower; it is populist, in and among the people and their problems, and it is as sensitive to issues of health as to issues of disease. It is as preoccupied with chronic as with infectious disease, with minorities and developing nations as with majorities in developed nations.
“Little-e” epidemiology is not universal or even a majority view. But it is a working-doing epidemiology as well as a conceptual, modeling epidemiology. And one of its credos is: “If it isn’t fun, it isn’t epidemiology!” (Henry Blackburn)
[The “little-e, big E” terminology is attributed to Roy Dawber, who hadn’t much truck with Big-E epidemiologists.]